Retinal Detachment
Definition of Retinal Detachment
Retinal Detachment is a separation of the retina (the inner nervous tunic of the eye) from the choroid (the middle, vascular tunic of the eye) in the back of the eye, usually resulting from a hole in the retina that allows the vitreous humor (fluid) to leak between the choroid and the retina.
Description of Retinal Detachment
The retina is a thin, transparent tissue of light-sensitive nerve fibers and cells. It covers the inside wall of the eye the same as wallpaper covers the walls of a room.
Most retinal detachments are caused by the presence of one or more small tears or holes in the retina. Normal aging can sometimes cause the retina to thin and deteriorate, but more often shrinkage of the vitreous body, the clear gel-like substance which fills the center of the eye, is responsible for deterioration and retinal tears. The vitreous is firmly attached to the retina in several places around the back wall of the eye. As the vitreous shrinks, it may pull a piece of the retina away with it, leaving a tear or hole in the retina.
Though some shrinkage of the vitreous body occurs naturally with aging and usually causes no damage to the retina, abnormal growth of the eye (sometimes a result of nearsightedness), inflammation or injury, may also cause the vitreous to shrink. In most cases, a significant change in the structure of the vitreous body occurs before the development of a retinal detachment.
Once a retinal tear is present, watery fluid from the vitreous space may pass through the hole and flow between the retina and the back wall of the eye. This separates the retina from the back of the eye and causes it to “detach.” The part of the retina that is detached will not work properly and there will be a blindspot in vision.
PRK
When patients read about laser vision correction they are presented with a multitude of names, acronyms, and abbreviations. Whether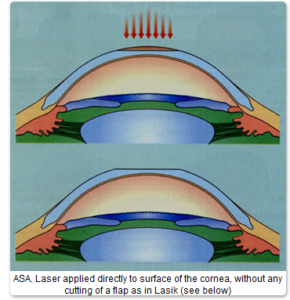 it’s LASIK, iLASIK, intraLASIK, PRK, LASEK, or epi-LASIK, it’s all extremely confusing even for the most enthusiastic patient who is about to undergo this life changing laser eye surgery. Is any technique really better than any other? How do doctors decide what to recommend, and how do you decide what to choose?
it’s LASIK, iLASIK, intraLASIK, PRK, LASEK, or epi-LASIK, it’s all extremely confusing even for the most enthusiastic patient who is about to undergo this life changing laser eye surgery. Is any technique really better than any other? How do doctors decide what to recommend, and how do you decide what to choose?
Laser eye surgery for vision correction works by reshaping the curvature of the transparent layer of the eye in front of the pupil, called the cornea. The laser evaporates corneal tissue elegantly and delicately, making it flatter in short sighted (myopic) people and steeper in the long sighted (hyperopic).
Overall there are really just two laser techniques, the difference being where on the cornea the laser is performed-either on the surface, or deeper under a thin flap of corneal tissue.
SURFACE TREATMENTS (PRK)
The first technique which can be called “surface treatment” as the laser affects the surface of the cornea directly, involves the gentle removal of the outer skin-like layer of cells called the epithelium, exposing the tissue below which then receives the laser. After the treatment there is a period of about 5 days when the eyes are uncomfortable, tender and watery with blurry vision as the epithelium grows back and the eye surface heals. The original name of this technique is Photorefractive Keratectomy or PRK and is the longest established laser technique with over 20 years follow up, stable long term results and is extremely safe. Many people also refer to PRK as ASA (Advanced Surface Ablation)
Epi-Lasik and LASEK are almost the same as PRK except both remove the epithelium in such a way (the former mechanically with a blunt instrument which slides across the eye, the latter with dilute alcohol which chemically loosens the tissue) that it can be replaced again afterwards. Some claim that by replacing the epithelium, recovery is more comfortable and may give better visual results especially with high prescriptions. These claims are controversial and not universally accepted, as tests have shown that the original epithelium tends to dissolve and is in any case replaced by fresh epithelium growing in.
The safety and ultimate vision are the same for all surface techniques- excellent .
UNDER A FLAP TREATMENTS (LASIK)
The second group of techniques used in laser vision correction involves cutting the cornea, and raising about 20% of the corneal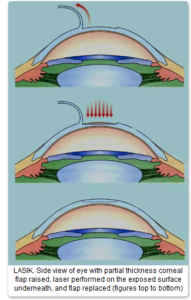 thickness as a flap on a hinge- and more invasive and complicated procedure. The big advantage is that as the laser treatment is under the flap which is immediately replaced after the laser ablation, and not exposed as in the surface treatments, recovery is much quicker, most seeing well the next day with no discomfort beyond the first few hours. The average cornea is slightly more than half a millimeter thick in the center (500microns) and the flap is usually between 100-160 microns in thickness, which is folded back on a hinge of uncut cornea (see diagram).
thickness as a flap on a hinge- and more invasive and complicated procedure. The big advantage is that as the laser treatment is under the flap which is immediately replaced after the laser ablation, and not exposed as in the surface treatments, recovery is much quicker, most seeing well the next day with no discomfort beyond the first few hours. The average cornea is slightly more than half a millimeter thick in the center (500microns) and the flap is usually between 100-160 microns in thickness, which is folded back on a hinge of uncut cornea (see diagram).
Most laser centers use an instrument called a microkeratome, which consists of a sharp oscillating and computerised blade that moves across the eye cutting the flap as it passes. This technique is called LASIK and is the most well known by today’s laser candidates. It is also extremely safe, although on the very rare occasions that a problem occurs during laser vision correction treatments, it is usually connected with the flap.
IntraLASIK uses a special laser (femtosecond laser) to cut the flap (and another laser machine to perform the actual treatment of removing the glasses prescription). Supporters of femtosecond laser claim that it is safer than an oscillating blade, and that it creates more accurate and thinner flaps. Some studies seem to support this, but in fact modern microkeratomes are also extremely safe, can also create thin flaps, and only very rarely cause complications- and even when they do, they rarely cause significant long term problems for the patient. There have been few studies comparing femtosecond laser with modern microkeratomes so the issue is still controversial. Also there have been on rare occasions complications with femtosecond laser flaps also. Femtosecond laser treatments are generally much more expensive. When the intralase laser is used to make the flap and paired with a (wavefront) Customvue VISX laser treatment it is also referred to as iLASIK, and marketed as such.
The main long term concern with LASIK and femtosecond Laser is that by cutting the cornea, it becomes structurally weaker. In about 1 in several thousand cases, and possibly much more frequently (exact figures are difficult to determine as not all cases are reported), after a few years the cornea can start to bulge out (a condition called ectasia) causing severe astigmatism, irreversible damage to vision and even a need for a corneal graft. Most at risk cases of ectasia can be predicted in advance e.g. candidates with thin corneas, irregularly shaped corneas, high prescriptions, and they can safely be offered a PRK surface treatment instead. But some cases occur for no obvious reason.
Conclusion
So what are the considerations when deciding which technique is best for you? Firstly of course any potential candidate needs to be assessed to make sure he is a good candidate for either technique. Some patients are only suited for surface treatment such as those with thin corneas, which makes the decision easier.
For patients who are good candidates for both techniques the choice is between two very safe and successful techniques, and both of which give equally superb results. Surface treatment (PRK) is a simpler operation but healing is slower requiring a few days off work (a small price to pay for the long term safety benefits) and vision takes a little longer to reach a good functioning level (5 days usually).
LASIK is a more complicated operation involving the cutting of a flap which is the main source of the rare problems that can occur during the laser vision correction procedure. There is also the issue of the very rare but serious long term problem of ectasia. But with more rapid healing, almost instant results and with little interruption in daily routine it continues to be very popular. Most patients are back to work or school the next day.
During a free consultation at Eye Care Surgery Center, we will check your prescription, measure your corneal thickness, and map the shape of your cornea which will allow him to make the proper recommendation for which treatment is best for you. Approximately 10-15% of patients at our clinic choose PRK surgery.

